|
Case of the Month: June 2026
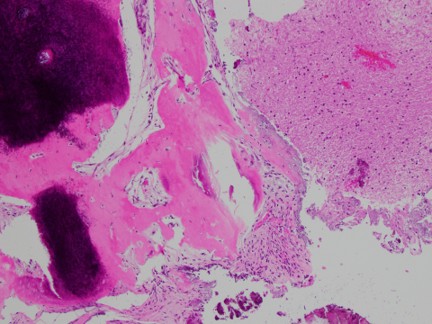
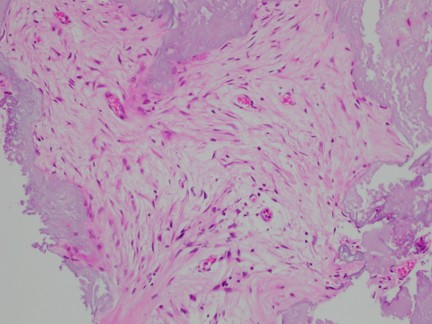
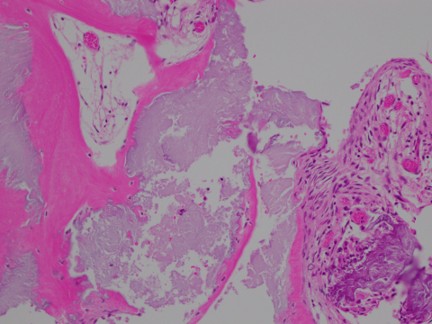
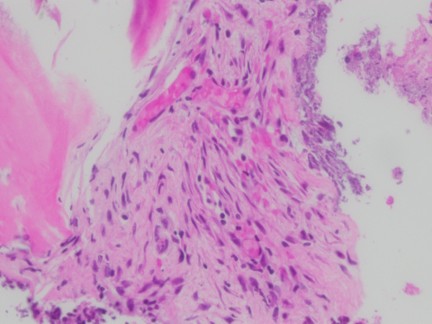
Title: A 62-year-old male with intractable seizures Authors: Maryam Abdo MD, Nelli S. Lakis MD Institution: The University of Kansas Health system Clinical History: A 62-year-old male presented to the emergency department with intractable seizures. Radiology: Magnetic resonance imaging (MRI) of brain showed densely calcified mass centered in the right centrum, semiovale along the deep precentral sulcus measuring 2.2 x 2.0 cm. The lesion demonstrated heterogeneous internal T2 hyperintensity and linear peripheral and heterogeneous internal enhancement. Representative Histology / IHC: Specimen was entirely submitted and examined. Histology from the resection showed predominantly a fibroosseous lesion associated with granular amorphous to chondromyxoid fibrillary cores with abundant calcification and ossification. The bone appeared non-neoplastic and surrounding some of the fragments are bland-appearing spindle to epithelioid cells with variable fibrous stroma. There was also some surrounding brain parenchyma (mostly detached & fragments), which is mildly hypercellular and gliotic. Immunohistochemical stains and special stains were performed; GFAP and IDH1-R132H highlighted the brain fragments while negative in the spindle cells. EMA, STAT6, Olig2, S100, SV40, GMS, B-amyloid, AFB were negative. CD68 highlighted scattered macrophages. Ki67 was low < 1%. Comprehensive next-gene sequencing showed no molecular abnormalities.
GFAP immunostain highlights the brain fragments while negative in the spindle cells.
Questions for Viewers: 1) What is the final diagnosis? 2) What are the important differential diagnoses? 3) What is the standard of treatment for this lesion? |

Our Sponsors
